
Economic Impact of Blood Transfusions





The Role of Diagnostic Point-of-Care Testing
“Diagnostic testing is an essential component of Patient Blood Management. The accurate assessment of the true causes of bleeding dysfunction facilitates the employment of evidence based, goal directed therapy to rapidly prevent and treat excess blood loss.”
Sherri Ozawa RN Clinical Director, Institute of Patient Blood
Management, Englewood Hospital Medical Center, Englewood, NJ
What Is the Issue?
Blood transfusion is the most common procedure performed in US hospitals 1
- Every year, approximately 14 million units of packed red blood cells are used2
- One in ten hospitalized patients who undergoes an invasive procedure is transfused3
- It is estimated that 40-60% of transfusions are administered without appropriate clinical justification4
Modifiable risks that can reduce patient exposure to blood products 5
94% of transfusions in surgical patients can be attributed to modifiable events.
- Low preoperative hemoglobin levels
- Excessive surgical blood loss
- Inappropriate transfusion practices
What Factors Impact Bleeding Related Complications?
Evolving technology in health care can predispose patients to bleeding complications.6
- Progressive widespread use of anticoagulant and antiplatelet therapeutics
- Technological advances that enable complex and lengthy surgical procedures
- Advancing age of the general population with associated comorbidities that predispose to bleeding related complications
Goals of Diagnostic Testing in Patient Blood Management
Rapid diagnosis and arresting blood loss by accurately assessing true causes of bleeding dysfunction8
- Use both quantitative and qualitative measures to assess true coagulation status
- Recognize the major mechanism of a developing coagulopathy
- Use goal directed diagnostic testing to direct and establish treatment goals
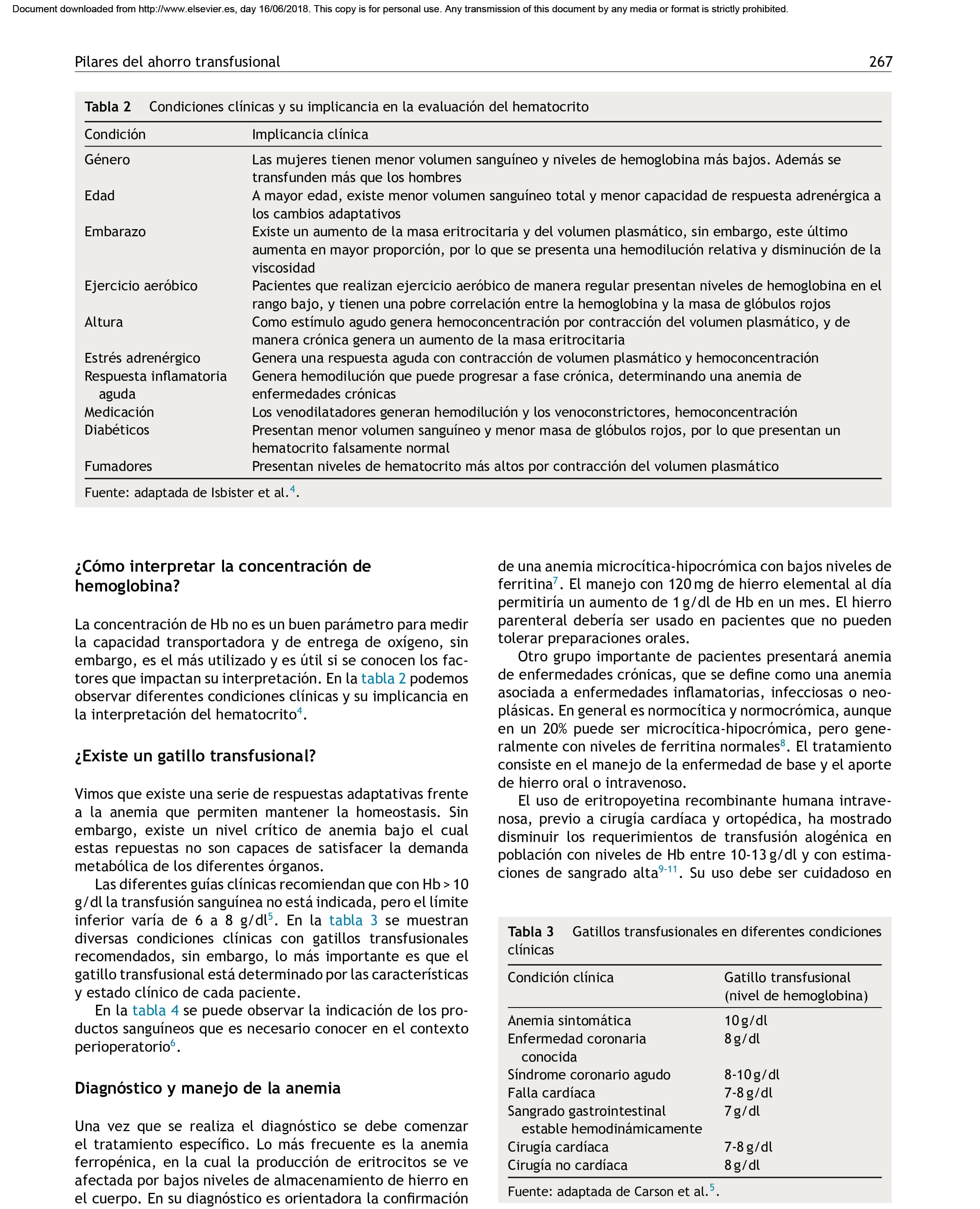
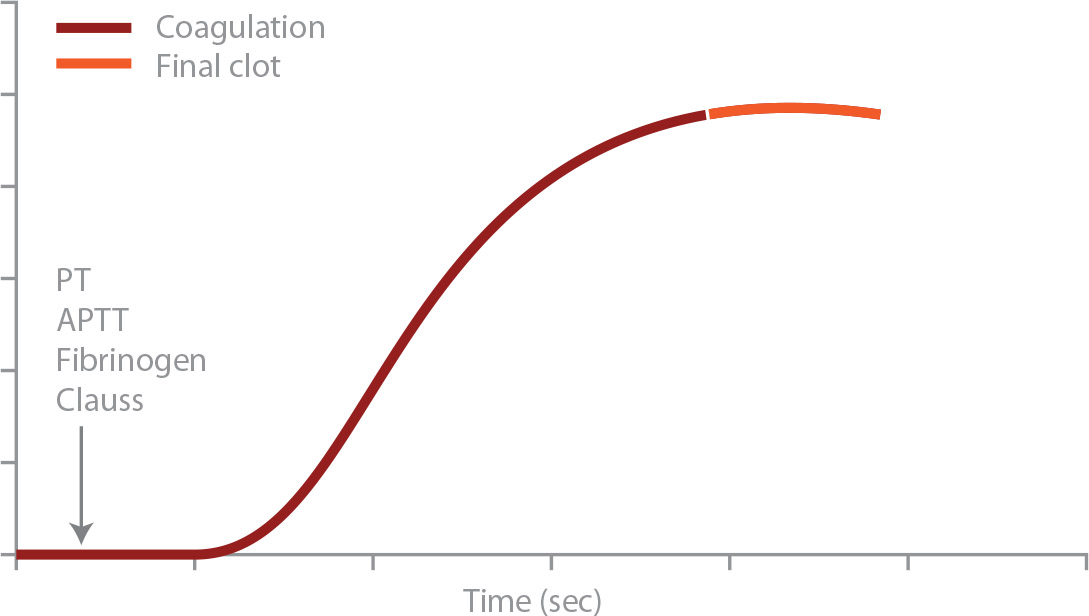
Conventional Coagulation Testing – What Do We See?
Blood tested almost one hour after it is drawn
Blood is drawn. It’s transported to the laboratory. It’s centrifuged. The cells are removed. Calcium and activators are added. Clot initiation (ATT and PTT) is measured.
Routine plasma coagulation tests only reflect 1-2% of the entire coagulation process9
- Only 5% of total thrombin has been generated when the coagulometer stops
- Only plasma is analyzed
- Interaction of platelets (or any other cells) are not assessed
- Interaction with the coagulation system, fibrinolysis or FXIII is not assessed
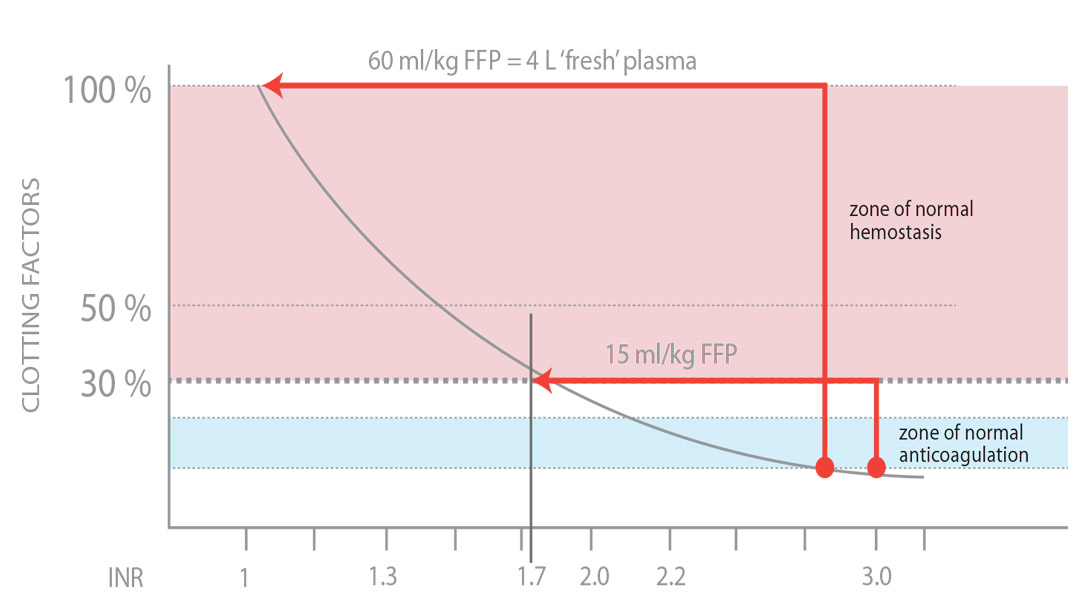
Mildly abnormal test results are associated with hemostatically adequate coagulation factor concentrations10
Below is a graph comparing the percentage of available clotting factors with INR values.
- 25-30% of factors are required to produce a clot (INR ≈ 1.7)
- INR may be elevated, but patient is still able to clot
Mildly abnormal test results are associated with hemostatically adequate coagulation factor concentrations10
Below is a graph comparing the percentage of available clotting factors with INR values.
- 25-30% of factors are required to produce a clot (INR ≈ 1.7)
- INR may be elevated, but patient is still able to clot
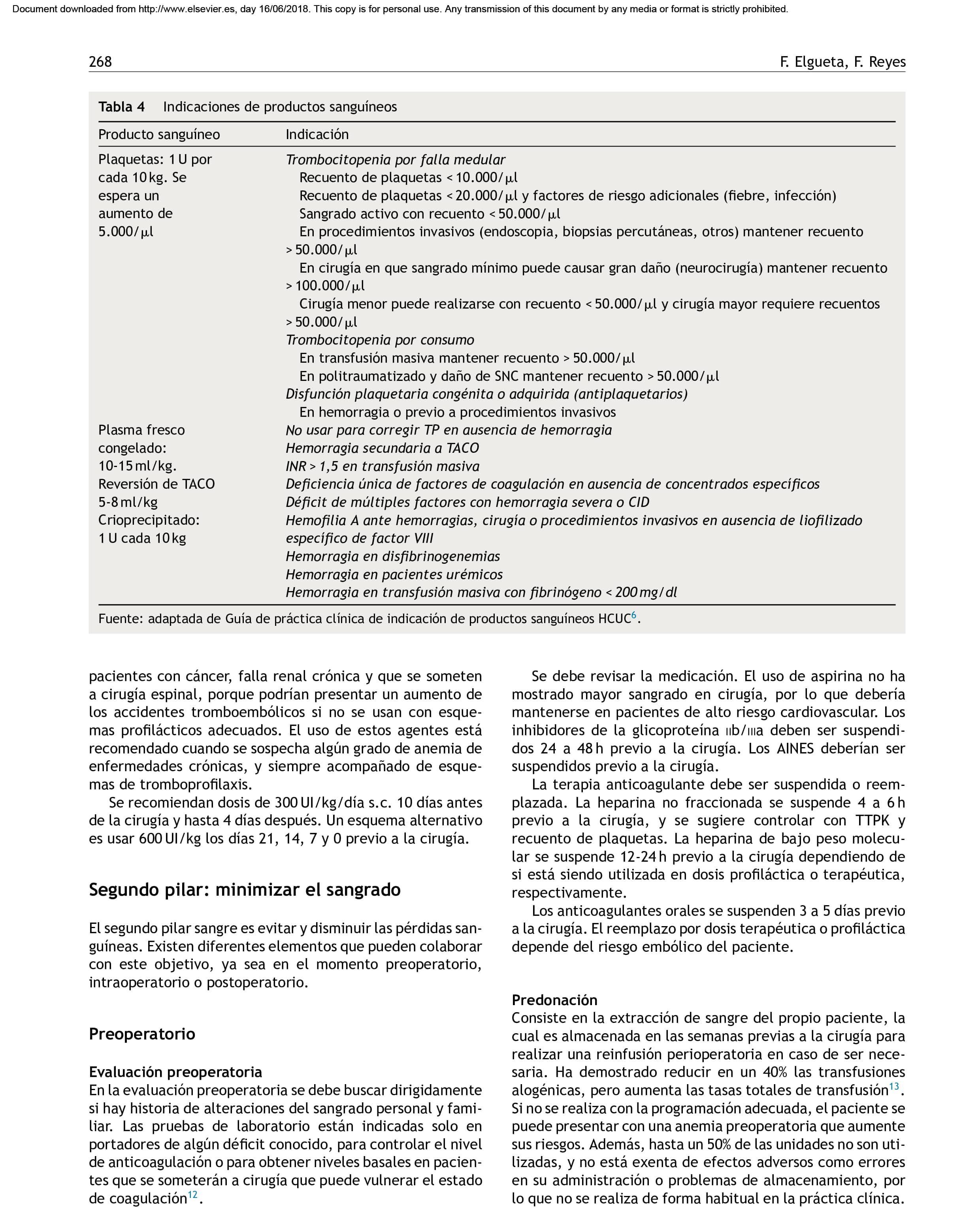
New Insights: Viscoelastic Diagnostic Testing
Basic principles of rotational thromboelastometry (ROTEM™)11
A citrated blood sample is placed is a stationary cup with calcium chloride and a coagulation activator. The rotating pin is lowered into the blood. Clot formation changes the torque between the pin and the cup.
Basic principles of rotational thromboelastometry (ROTEM™)11
A citrated blood sample is placed is a stationary cup with calcium chloride and a coagulation activator. The rotating pin is lowered into the blood. Clot formation changes the torque between the pin and the cup.
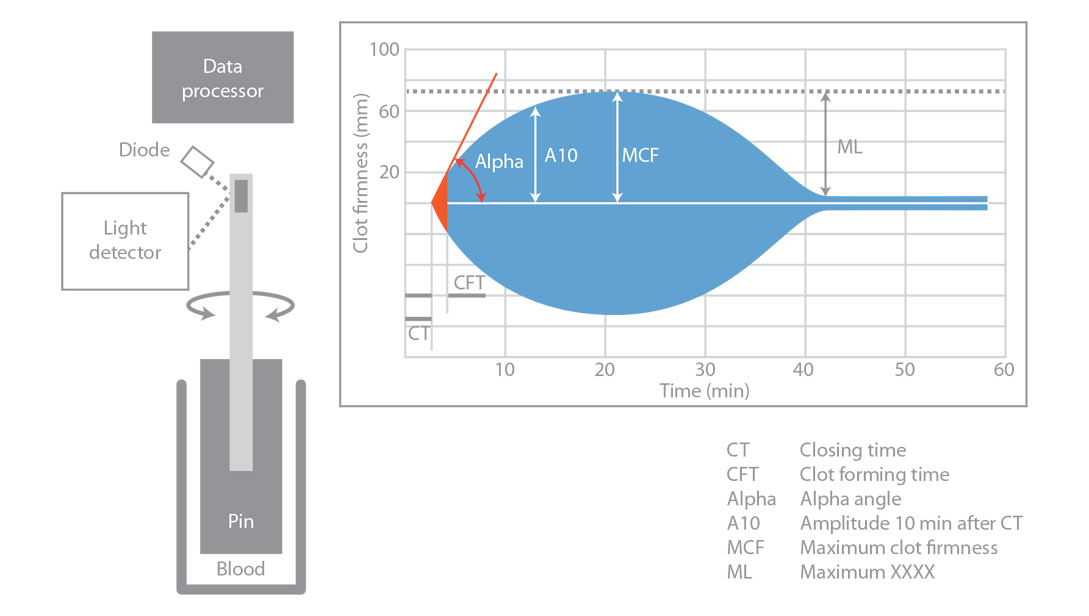
Measurements include coagulation time (CT;sec), clot formation time (CFT; sec), -angle (degrees), amplitude at 10 minutes after CT (A10; mm), maximum clot firmness (MCF; mm), and maximum lysis (ML; % decrease decrease 60 min after MCF).
Morphology and clot formation changes are dependent on clotting defect11
Below are examples of ROTEM™ traces using the EXTEM test.
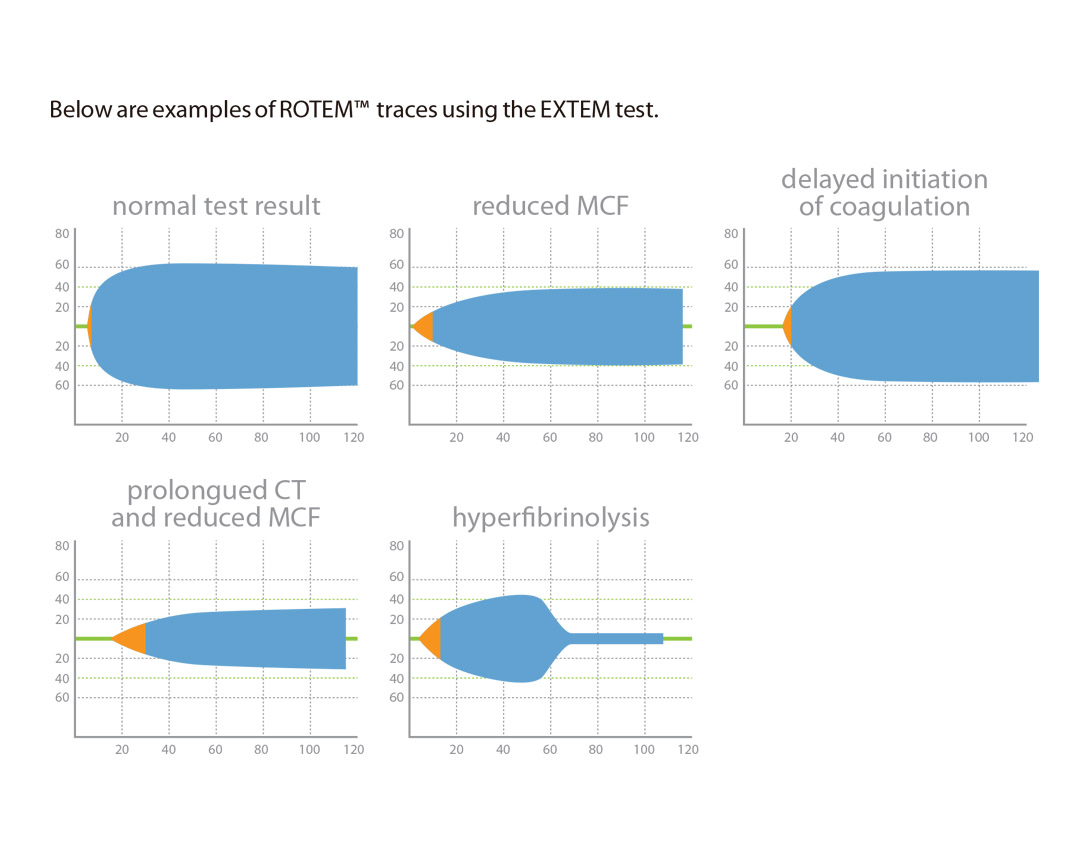
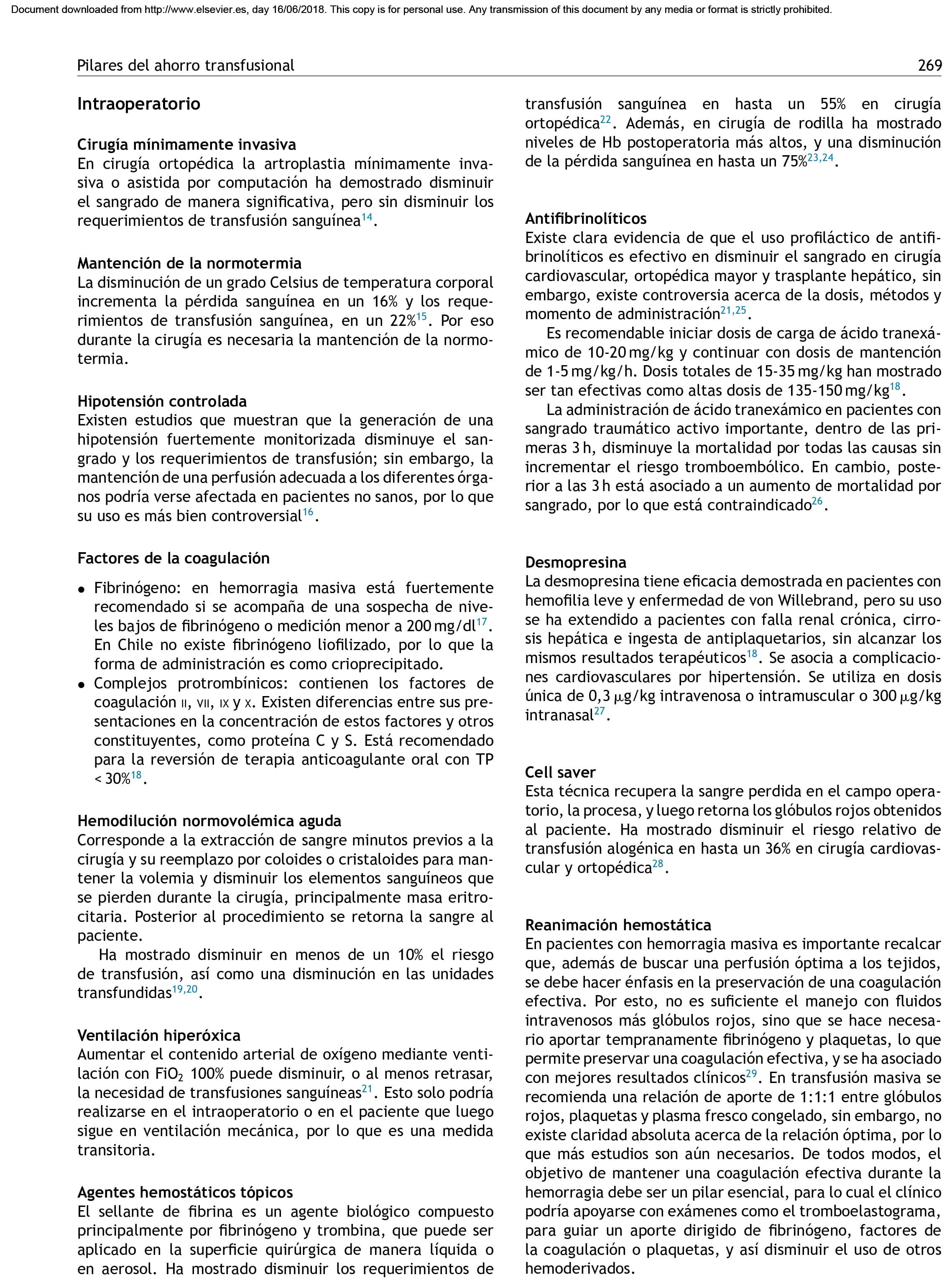
Allows assessment of clotting defect and replenishment of what is needed without additional blood components
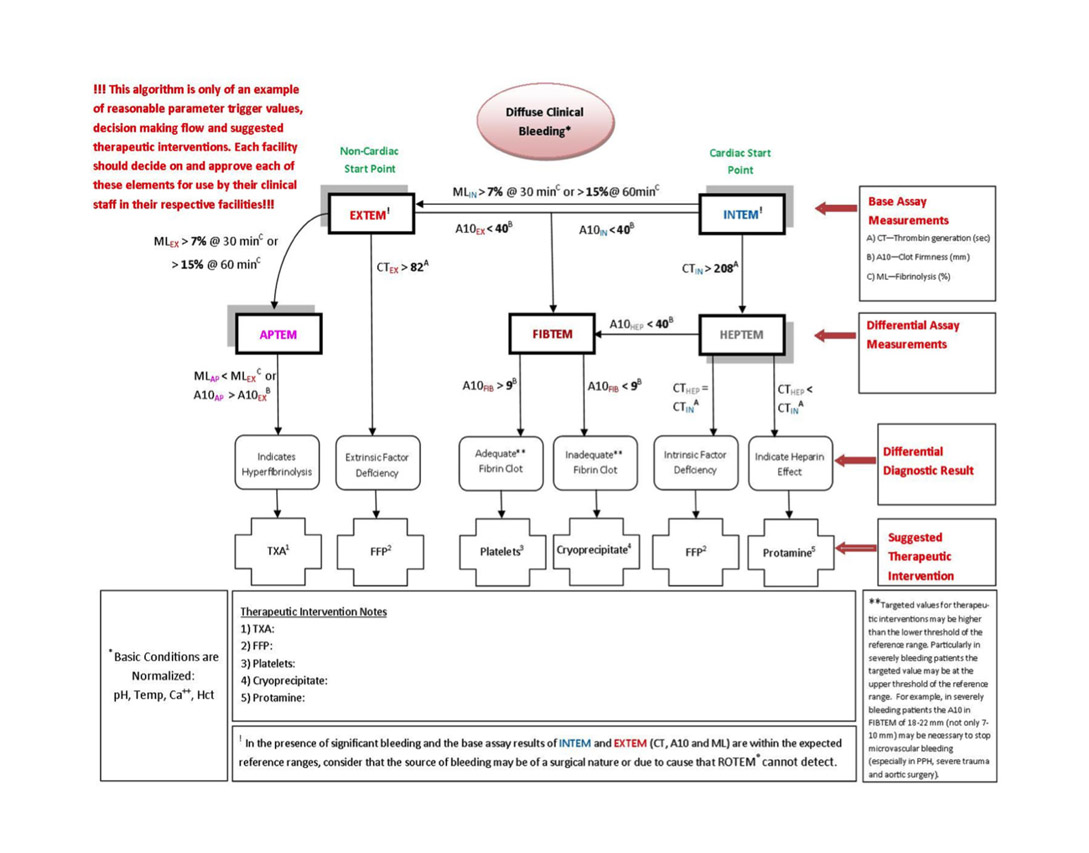
Below is an algorithm using the results of viscoelastic testing and a summary of therapeutic options.
Viscoelastic POC Testing (TEG®) guided therapy was superior to conventional coagulation tests in trauma patients12
Holcomb (2012) evaluated a series of 1974 trauma patients, 25% of whom presented in shock and 28% of whom were transfused. The authors found that TEG®, Haemonetics®, predicted RBC transfusion and massive transfusion better than PT or PTT. TEG® was superior to fibrinogen in predicting plasma transfusion, and superior to platelet count in predicting platelet transfusion.
Advantages compared to conventional coagulation testing11,13
- Conventional coagulation testing only provides limited information on the underlying coagulation disorder
- Whole-blood viscoelastic tests such as rotational thromboelastometry (ROTEM) or thrombelastography (TEG) offer a more comprehensive insight into the coagulation process in trauma
- Results are available within minutes and they provide information about:
- Initiation of coagulation, the speed of clot formation, and the quality and stability of the clot
- Viscoelastic tests have the potential to guide coagulation therapy according to actual needs of each patient and reducing the risks of over or under transfusion
- Goal-directed therapy with specific hemostatic drugs, coagulation factor concentrates, and blood components
- In several cohort studies, this POC-based management was associated with:
- Reduced transfusion requirements
- Reduced incidence of transfusion associated adverse events
- Improved patient outcomes
Summary
The superior information obtained with viscoelastic testing is critical to better direct effective therapeutic interventions in patients with coagulation issues. Optimizing coagulation is a fundamental principle of Patient Blood Management and along with other evidence based interventions, can positively impact patient outcome. Implementing organized PBM programs, which incorporate advanced capabilities such as viscoelastic testing result in better clinical decision making, cost savings, and optimal patient care.
What is Patient Blood Management?
“The timely application of evidence based medical and surgical concepts designed to manage anemia, optimize hemostasis, and minimize
blood loss in order to improve patient outcomes.” – Society for the
Advancement of Blood Management (SABM.org)
References
- Agency for Healthcare Research and Quality. Healthcare Cost Utilization Project Statistical Brief. #149.Most Frequent Procedures Performed in Hospitals 2010. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb149.pdf – Accessed July 18, 2013.
- Department of Health and Human Services, National Blood Utilization and Collection Survey, http://www.hhs.gov/ash/ bloodsafety/nbcus/index.html
- Agency for Healthcare Research and Quality. HCUP Facts and Figures: Statistics on Hospital-Based Care in the United States, 2007. Available at: http://www.hcup us.ahrq.gov/reports/factsand”gures/2007/ pdfs/FF_report_2007.pdf – Accessed June 16, 2013.
- Shander A, Fink A, Javidroozi M, Erhard J, et al.Appropriateness of allogeneic red blood cell transfusion: the international consensus conference on transfusion outcomes. Transfus Med Rev. 2011 Jul;25(3):232-246.e53
- Shander A, Javidroozi M, Perelman S, et al Mt Sinai J Med. Jan-Feb 2012.
- Shander A, kaplan L, Harris M et al. Topical Hemostatic Therapy in Surgery: Bridging the knowledge and Practice Gap J Am Col Surg. 2014; in press.
- Stokes ME, ye X, Shah M, Mercaldi k, Reynolds MW, Rupnow MF, Hammond J. Impact of bleeding-related complications and/or blood product transfusions on hospital costs in inpatient surgical patients. BMC Health Serv Res. 2011; 11:135.
- Armand R, Hess JR. Treating coagulopathy in trauma patients. Transfus Med Rev. 2003; 17(3): 223-31.
- Mann kG, Brummel k, Butenas S. What is all that thrombin for? J Thromb Haemost. 2003 Jul;1(7):1504-14.
- Dzik WH, in Mintz PC ed. Transfusion Therapy: Principles and Practice, 2nd edition. AABB 2005
- Schöchl H, Maegele M, Solomon C, Görlinger k, Voelckel W. Early and individualized goal-directed therapy for traumainduced coagulopathy. Scand J Trauma Resusc Emerg Med. 2012 24;20:15.
- Holcomb JB, Minei kM, Scerbo ML, Radwan zA, Wade CE, kozar RA, Gill BAlbarado R, McNutt Mk, khan S, Adams PR, McCarthy JJ, Cotton BA. Admission rapid thrombelastography can replace conventional coagulation tests in the emergencydepartment: experience with 1974 consecutive trauma patients. Ann Surg. 2012 Sep;256(3):476-86.
- Lier H, Vorweg M, Hanke A, Görlinger k. Thromboelastometry guided therapy of severe bleeding. Essener Runde algorithm. Hamostaseologie. 2013;33(1):51-61.